Waardenburg syndrome is a rare disease characterized by deafness in
association with pigmentary anomalies and defects of
neural crest-derived tissues1.
Above mentioned case was first reported in 1951, by a
geneticist P. J. Wardenberg who potrayed
it along with the 6 main features. Those features are Lateral displacement of
the medial canthi combined with dystopia of the lacrimal puncta
and blepharophimosis, Prominent broad nasal root, Hypertrichosis of the medial part of the eyebrows, White
forelock, Heterochromia iridis,
Deafmutism2.
Waardenberg syndrome is divided into four sub types; this division is
based on the presence and absence of dystopia canthorum
along with other certain clinical features. These subtypes are WS1,
WS2, WS3 and WS4. It affects equally both
sexes and all races3.
It is estimated that 1 per 10,000 - 20,000 people are
diagnosed with waardenberg syndrome, with a
prevalence rate of approximately 1 in 10,000 or 0.01% in US4.
Among four types of syndrome, I and II are the most common,
whereas types III and IV are rare.
Five
major and five minor criteria exist for diagnosing WS. The major criteria are sensorineural hearing loss, iris pigmentary
abnormality (two eyes different color or iris bicolor or characteristic
brilliant blue iris), hair hypopigmentation (white forelock or white hairs at
other sites on the body), dystopia canthorum (lateral
displacement of inner canthi) and the presence of a first-degree relative
previously diagnosed with WS. The minor criteria are skin hypopigmentation
(congenital leukoderma/white skin patches), medial
eyebrow flare (synophrys), broad nasal root,
hypoplasia of alae nasi,
and premature graying of hairs (before age 30)3.
CASE REPORT
Our first patient is a 22 year old male presented to the
outpatient department of our tertiary eye care hospital with chief complaints
of difference in color of his eyes with decreased vision in right eye (Fig. 1).
His Best corrected visual acuity at presentation was 6/24 p OD with -3.50 x
-1.00 at 90 degree and 6/6 OS. Patient also has complain
of decreased hearing in right ear. He was the last child of a
non-consanguineous marriage among 7 siblings with one affected brother as well.
(3 brothers and 3 sister). His birth and developmental
history did not reveal anything significant. His detailed family history
revealed that his mother has telecanthus along with 1
brother and 2 nephews and 2 nieces affected as well.
On systemic examination, he was
moderately built with an average height, weight and normal IQ. He had premature
graying of hair with absence of any associated depigmentation elsewhere on the
body. His ENT and abdominal examinations were normal.
On ocular examination, gross inspection
shows broad nasal root and synophrys. The palpebral
fissure height of right eye was 1.5 cm and 1.4 cm in left eye along with
lateral displacement of canthi. He also had dystopia canthorum
with interpupillary distance of 8cm and inner canthal distance of 5.7 cm. Hirschberg corneal reflex was
central but medially sclera was visible o a lesser extent.
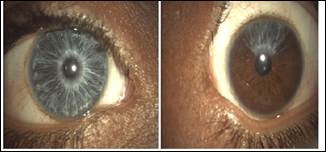
Complete heterochromia
due to hypoplastic iris, blue in color was noted in
right eye (Fig. 2). Sectoral atrophy of iris seen in
left eye. Besides this anterior segment examination was otherwise normal in
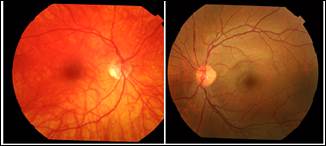
both the eyes. IOP was in normal limits. Pupillary reactions were normal. Right
fundus was albinotic showing hypopigmentation and
temporal disc pallor and left fundus was normal (Fig. 3). Gonioscopy
revealed grade IV angle in both eyes, normal iris vessels seen in angle of
right eye.

Fig. 1: Shows telecanthus.
Right Eye Left Eye
Fig. 2: Shows anterior
segment
Right
Eye Left Eye
Fig. 3: Shows right hypopigmented fundus
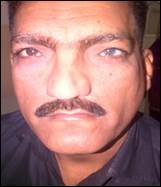
Fig. 4: Shows telecanthus, synophrys and heterochromia left
eye

Right Eye Left
Eye
Fig. 5: Anterior
segment
2 children of elder brother (our 3rd and 4th
patient) showed only telecanthus and broad nasal root
in examination with rest of the examinations normal.
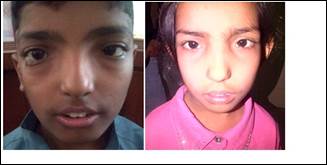
Nephew Niece
Fig. 6: Shows telecanthus
and broad nasal root.
Our second patient is 46 years old male, elder brother of
patient. His history revealed presence of white forelock of hairs at birth (due
to hair dying at early age patient has no old picture) and premature graying of
hairs, dystopia canthorum, synophrys
and heterochromia irides.
His visual acuity was 6/6 in both eyes. Right eye shows sectoral
iris atrophy and complete heterochromia found out in
left eye. Both fundii were normal.
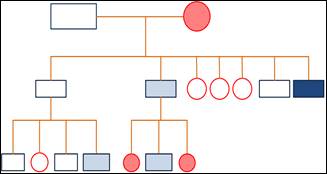
Fig. 7: Pedigree chart.
Dark blue box: first patient. Light
blue box: other affected males. Red circles: affected females.
DISCUSSION
Waardenburg consortium proposed diagnostic criteria for diagnosing WS
types. According to it, for placing patient in category of WS I, patient should
have 2 major or 1 major + 2 minor criteria present. WS II is characterized by
sensor neural hearing loss and heterochromia iridis but absence of dystopia canthorum.
WS III (Klein–Waardenburg syndrome) resembles type I
with supplementary musculoskeletal abnormalities. These patients have hypoplastic muscles and contractures of the upper limbs. WS
IV is associated with Hirschsprung disease. Liu et al. suggested method for diagnosis of WSII, which
requires presence of at least two major criteria and the same study propounded
the use of premature graying as one of the mature criteria instead of dystopia
canthorum5.
We present a case series of a single family with several
members affected of first and second generation. According to the above
mentioned criteria our first and second patient falls in category of WS 1.since
all of these are only cosmetic problems therefore they do not require
compulsory treatment.
It
is plausible that in certain cases WS may remain undiagnosed until other family
members with similar features seek medical attention. One of the purposes to
present this case series is to bring in light the significance of detailed
examination of all the family members to recognize undiagnosed cases. Clinical
features of WS are mainly cosmetic problems for which no definitive treatment
exist, except for few occuloplastic procedures which
can be done for broad medial canthus. In some cases muted diseases, such as, Sensorineural deafness, bony
abnormalities or Hirschsprung disease are found to be
associated with WS which results in deterioration in quality of life. An
ophthalmologist can help these patients by making an early diagnosis which may
aid in the initiation of early treatment, social and vocational training, and
rehabilitation of these patients.
ACKNOWLEDGEMENT
We
would like to express our special thanks to Prof. Hassan Niazi
for his valuable guidance and advise during diagnosis
and workup of this patient.
Author’s Affiliation
Dr. Nausheen
Hayat
Ophthalmology Ward
Jinnah Post Graduate Medical Centre
Karachi
Dr. Alyscia Cheema
Head of Department
Ophthalmology Ward
Jinnah Post Graduate Medical Centre
Karachi
REFERENCES
1.
Eglabian F. Waardenberg-Shah syndrome; a
case report and review of literature. Iran J Pediatr.
2008; 18: 71-4.
2.
Waardenberg PJ. A new syndrome combining developmental anomalies of the
eyelids, eyebrows and nose root with pigmentary
defects of the iris and head hair and with congenital deafness. Am J Hum Genet.
1951; 3: 195-253.
3.
Ghosh SK, Bandyopadhyay D, Ghosh A, Biswas SK, Mandal RK. Waardenberg syndrome: a report of
three cases. Indian J Dermatol Venereol
Leprol. 2010; 76: 550-2.
4.
Right diagnosis.com. Denver (CO):
Health Grades Inc; 2011. Statistics by country for Waardenberg
syndrome. 2013; 7.
5.
Bansai Y, Jain P, Goyal G, Singh M, Mishra C. Waardenberg syndrome-a case
report. Clae. 2012; 36: 49-51.